 Joep Perk 瑞典Linnaeus 大学健康科学系教授
Joep Perk 瑞典Linnaeus 大学健康科学系教授
Atherosclerotic CVD remains the leading cause of premature death worldwide. It affects both men and women: Each year in Europe over 4.3 million people will die of CVD (source: European Heart Network). CVD is estimated to be responsible for 42% of deaths before the age of 75 years in women and 38% in men. The vast majority of these deaths might have been prevented through the widespread adoption of simple interventions such as smoking cessation, improved diets, and increased exercise.
The 2012 version of the “European Guidelines on Cardiovascular Disease Prevention in Clinical Practice ” were produced by the Fifth Joint European Societies Task Force (5th JTF), which includes cardiologists, general practitioners, nurses, and experts from the field of atherosclerosis, hypertension, diabetes mellitus, stroke, behavioural medicine and from non-governmental organisations. The guidelines are designed to be more accessible, in order to help disseminate the information to health professionals working in the field. At the beginning of each chapter, the JTF has isolated and condensed the recommendations, the most important new information, and remaining gaps in the existing scientific evidence to "key messages" that can be incorporated into practice easily. The document provides guidance using both traditional recommendation classes (I, IIa, IIb, or III) according to the type of trial the evidence came from, and the Grading of Recommendations Assessment Development and Evaluation (GRADE) system which gives increased weight to population studies.
What is CVD prevention?
“A coordinated set of actions, at public and individual level, aimed at eradicating, eliminating, or minimizing the impact of cardiovascular diseases and their related disability. The bases of prevention are rooted in cardiovascular epidemiology and evidence-based medicine.”
For whom is CVD prevention needed?
Risk factor screening should be considered in adult men ≥40 years and in women ≥50 years of age or if postmenopausal. Total risk estimation using multiple risk factors (such as the SCORE algorithm) is recommended for asymptomatic adults without evidence of CVD. While the physician in general practice is the key to initiating and coordinating long-term CVD prevention, nurse-coordinated prevention programmes should be well integrated into preventive healthcare systems.
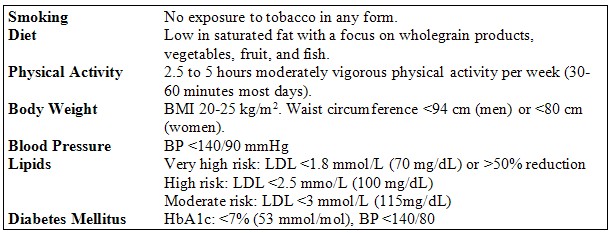
Using the SCORE algorithm, four levels of risk have been established with recommendations for each. The SCORE model uses age, gender, smoking habits, blood pressure and total cholesterol. There are different models for high risk and low risk countries and tables corrected for HDL-cholesterol levels. The electronic version is available at www.heartscore.org .
In the new guidelines, greater emphasis has been placed on the behavioural aspects of prevention, with a discussion of ways to make it easier for patients to change their lifestyles and a section exploring why patients do not adhere to medications.
Where should programmes be offered?
All patients with CVD must be discharged from the hospital with clear, guideline-orientated treatment recommendations. Patients after an acute ischaemic event should participate in a cardiac rehabilitation programme to improve prognosis by modifying lifestyle habits and increasing treatment adherence.
The final chapter focuses even on the “new era” of political engagement in preventive cardiology. In addition to clinical prevention activities, health care professionals?should extend their activities to include political lobbying for changes that influence healthy behaviours in the wider population.
Finally, the guidelines are available in full text at the website of the European Society of Cardiology (ESC) (www.escardio.org ). In addition to CME questions, key messages, and a dedicated slide set free for teaching purposes, a pocket version of the guidelines and a one page leaflet for use in general practice around Europe is available for order via the website.
核心信息
1、新指南强调心血管病预防应当从生命早期开始,直至死亡。
2、新指南更强调生活方式在预防中的重要地位,并寻求有效的方法使患者更易改变他们的生活方式。
3、新指南彻底颠覆了旧版指南的表达方法,力求更为简洁明了。
4、新指南采用了新的GRADE系统以评价研究证据,推荐类型只分为强推荐和弱推荐两类。
5、新指南更重视人口研究的数据。